Red Light Therapy for Papulopustular Rosacea
The "acne-looking" rosacea subtype that's often misdiagnosed — and often prescribed the wrong treatments. Red light therapy targets the inflammation and bacteria driving the bumps without the harsh side effects of oral antibiotics.
Quick Facts
Understanding Papulopustular Rosacea (PPR)
Papulopustular rosacea — "PPR" — is the subtype most commonly confused with adult acne. It affects roughly 25% of rosacea sufferers and features acne-like papules (firm red bumps) and pustules (pus-filled spots) that appear on the central face, alongside the persistent redness of rosacea.
Unlike acne, PPR bumps don't have blackheads or comedones. They appear symmetrically across the cheeks, nose, chin, and forehead, and they flare up in response to typical rosacea triggers (stress, alcohol, heat) — not clogged pores. Standard acne treatments like benzoyl peroxide often make PPR dramatically worse.
Common Symptoms
Critical distinction: If you've been treating "adult acne" for years with zero improvement (or worsening), you likely have PPR — not acne. A dermatologist can confirm with a simple skin exam.
How Red Light Therapy Clears PPR Bumps
PPR has three distinct drivers: chronic inflammation, elevated demodex mite populations, and bacterial overgrowth in inflamed pores. Red light therapy addresses all three — and uniquely, it's one of the only PPR treatments that includes safe blue light (480nm) for its antibacterial effect.
Reduces Cathelicidin (LL-37) Overproduction
PPR skin has abnormally high levels of cathelicidin — an antimicrobial peptide that paradoxically drives the inflammatory bumps rather than protecting against them. Photobiomodulation at 630–660nm has been shown to downregulate LL-37 expression, reducing new papule formation within 4–6 weeks.
Antibacterial Blue Light (480nm) Effect
Unlike ETR (where you turn off blue light), PPR benefits from gentle 480nm exposure. Blue light targets porphyrins in C. acnes and other bacteria implicated in PPR, killing them without the skin-barrier damage caused by benzoyl peroxide or harsh antibacterial washes.
Reduces Demodex Mite Population
Research suggests photobiomodulation disrupts the reproductive cycle of Demodex folliculorum mites — which are found at significantly elevated levels in PPR skin. This is part of why PPR responds to ivermectin (Soolantra), and RLT provides a complementary mechanism without prescription drugs.
Accelerates Healing of Existing Papules
Red light at 660nm and near-infrared at 830nm stimulate fibroblast activity and increase ATP production, helping existing bumps resolve faster — typically within 3–5 days instead of 10–14 days. This also reduces post-inflammatory hyperpigmentation after bumps heal.
Exact Dosing Protocol for PPR
PPR dosing differs from ETR — you can use blue light and go slightly more aggressive since bacterial/inflammatory targets respond well to higher doses.
Closer Than ETR Protocol
PPR can tolerate 10" from the start — the added intensity helps target bacteria and demodex more effectively. Move to 8" after 3 weeks.
Longer Sessions Accepted
Start at 10 minutes per side, build to 15 minutes. PPR doesn't have ETR's vascular fragility, so longer doses work well.
Daily Is Acceptable
PPR tolerates 5x weekly from week 1, and daily use from week 4 once skin adjusts. Take Sunday as a rest day.
Include Blue Light!
Unlike ETR, PPR benefits from 480nm blue for its antibacterial effect. Add 660nm if your device offers it — helps accelerate bump healing.
Flexible Scheduling
PPR isn't light-time sensitive like ETR. Morning works best for daily consistency, but evening sessions are equally effective.
Cleanse → Moisturize
Rinse with lukewarm water after sessions to wash off bacterial debris. Apply ceramide moisturizer. Skip toner and actives on RLT days.
Your PPR Clearing Timeline
PPR takes slightly longer to resolve than ETR because existing bumps need to heal AND new bump formation needs to stop. Here's the realistic timeline:
Initial "purge" possible
Some users experience a brief worsening as deeper bumps surface and clear. This resolves by week 3. Existing papules heal 30–40% faster than usual.
Fewer new bumps forming
The rate of new papule formation drops noticeably. Your "bump count" on any given day starts decreasing.
Visible clearing underway
Pustules resolving rapidly. Cheek texture improving. Background redness from PPR inflammation reducing. Post-inflammatory marks fading faster.
Major improvement
Most users report 60–80% reduction in active lesions. Skin texture smoother. Flares less frequent and milder when they happen.
Long-term maintenance
Drop to 3–4 sessions weekly. Reintroduce gentle actives (azelaic acid, niacinamide). Most PPR users maintain remission on this schedule.
Before & After: PPR Sufferers Using Red Light Therapy
Real Reddit users with papulopustular rosacea who followed consistent RLT protocols.
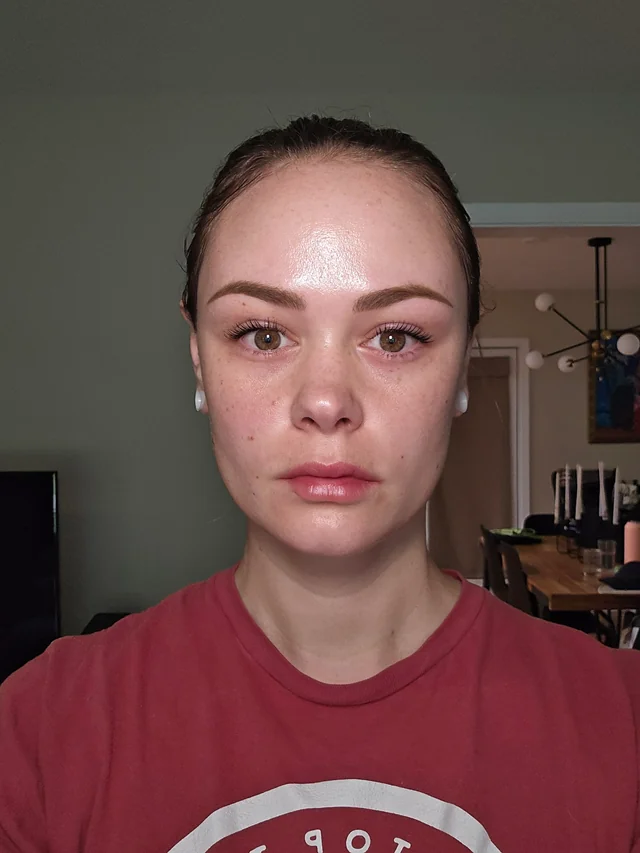

Active lesions reduced ~75%
Papule count dropped dramatically after 8 weeks of daily 10" / 12-minute sessions with 480 + 660nm combination protocol.


From constant breakouts to clear
User reports transitioning off oral doxycycline successfully after 12 weeks of RLT + topical azelaic acid routine.
Top 5 Red Light Devices for Papulopustular Rosacea
For PPR, you specifically want devices that include 480nm blue for antibacterial action — which narrows the field.

TotalSpectrum 3.0
Includes 480nm blue · 7 wavelengths · Acne-focused preset mode
Why it's #1 for PPR specifically
RLT Home is the ONLY top-5 panel with both 480nm blue and dedicated "Acne" preset mode — critical for targeting the bacterial component of PPR. You can turn on blue light specifically when you're treating active breakouts, then turn it off once clear.


Platinum LED — BIOMAX 900
480nm blue included · 7 wavelengths · broad spectrum
Why it ranks for PPR
Also includes 480nm blue in its spectrum, making it PPR-suitable. The broad wavelength range means you can target bacteria, inflammation, and healing simultaneously.


Rojo — Refine 3600
No 480nm · strong red + NIR inflammation control
Why it ranks for PPR
No 480nm blue, but the strong 630/660 + NIR protocol effectively targets inflammation and demodex. Pair with a separate $30 blue light mask for the bacterial component if using this device.
Helio Cure — Helio Blaze
No blue light · gentle for mixed PPR+ETR cases
Why it ranks for PPR
Best for users with both PPR and ETR features — the lower irradiance + no blue approach works well if you're more worried about triggering flushing than maximum bacterial kill.


Rouge Care — Ultimate G4
8 wavelengths · individually dimmable · no 480nm
Why it ranks for PPR
No blue light, but the 8-wavelength customization is powerful for targeting demodex and deep inflammation. FDA-cleared and clinically used for inflammatory skin conditions.
Common Questions About RLT for PPR
Why does my PPR get worse with acne treatments?
Can I use RLT alongside oral antibiotics like doxycycline?
Will blue light make my rosacea redness worse?
What if I have both PPR and ETR features?
How does RLT compare to Soolantra (ivermectin cream)?
Do I need blue light or is red enough?
Will my post-inflammatory marks fade faster with RLT?
Ready to Clear Your PPR?
Read our complete evidence-based rosacea guide, see more before/afters, and get the full device comparison.
See Top 5 Devices →